This post is an honest attempt to look at the COVID-19 vaccine from both sides. To get the vaccine or not, that is the question.
I am not an anti-vaccer, nor am I anti-humanity (which has been suggested as I won't just be vaccinated for the "common good"). I am cautious. I am a researcher. I have spend the last 37 years researching different subjects. I look at both sides, the following list is my research. Numbers correspond to sections below.
3. Government Recommendations
4. Dr. Fauci
4A. Shane Crotty PhD. on Dr. Fauci (positive interview)
4B. Dr. Fauci Interviewed on the Carlos Watson Show (positive interview)
4C. Interview with Judy Mikovits, PhD. on Dr. Fauci (opposing viewpoint)
4D. Articles on Dr. Fauci and the Vaccination of Children
4E. So much more on Dr. Fauci
5. The History of mRNA
7. World Health Organization - Fatality Rate From COVID19
9. America Frontline Doctors
12. Long-Term Vaccine Effects: Inflammation-induced Disruptions
13. World Health Organization - Infection Rate After Vaccine
14. Will Vaccines Save Lives?
15. COVID-19 Vaccine Side Effects - Concerned Doctors Speak Out
16. Are COVID19 Vaccines Gene Therapy?
17. What is Herd Immunity?
18. We are going to pay a huge price for mass COVID vaccination + Rebuttal
19. Corticosteroids & Ivermectin?
20. Dr. Suneel Dhand - Why I haven't taken the COVID vaccine yet
21. How Long After a COVID Diagnosis Should I Get Vaccinated? And other scenarios
22. 18 Reasons Why I Won't Get the COVID-19 Vaccine
23. How a False Hydroxychloroquine Narrative was Created by Dr. M. Nass and the Allegiance for Human Research Protection
24. Heart Inflammation After COVID Vaccine
25. The Many Ways in Which COVID Vaccines May Harm Your Health
28: US Spending $1.2 billion on Merck's COVID-19 Treatment Is a 'Waste of Taxpayers' Money' (
29. CDC Finds 'LIkely' Link between Heart Inflammation and Pfizer, Moderna COVID Vaccines
30. The COVID Spike Protein and the Still Uncertain Side Effects of the mRNA Vaccines
***31. Might COVID Injections Reduce Lifespan?
Interview with Patrick Coffin
August 2021
PLEASE WATCH HERE
May 19, 2021
an interview with Patrick Coffin June 2021
Podcast #234 Top Cardiac Doctor Warns Against the Vaccine
Watch Video Here from Stew Peters
Data released today by the Centers for Disease Control and Prevention (CDC) showed that between Dec. 14, 2020 and Sept. 3, 2021, a total of 675,593 adverse events following COVID vaccines were reported to the Vaccine Adverse Event Reporting System (VAERS). The data included a total of 14,506 reports of deaths — an increase of 595 over the previous week.
There were 88,171 reports of serious injuries, including the reports of deaths, during the same time period — up 2,200 compared with the previous week.
August 13, 2021
Data released today by the Centers for Disease Control and Prevention (CDC) showed that between Dec. 14, 2020 and Aug. 13, 2021, a total of 595,622 total adverse events were reported to VAERS, including 13,068 deaths — an increase of 702 over the previous week.
There were 81,050 reports of serious injuries, including deaths, during the same time period — up 10,945 compared with the previous week.
Excluding “foreign reports” filed in VAERS, 464,769 adverse events, including 6,018 deaths and 37,806 serious injuries, were reported in the U.S. Of the 6,018 U.S. deaths reported as of Aug. 13, 13% occurred within 24 hours of vaccination, 19% occurred within 48 hours of vaccination and 33% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
This year as of June 4th there have been 5,888 COVID vaccine related deaths (my brother-in-law was one of these), and 652 miscarrages. See the above link for more information.
Hospitalized or fatal COVID-10 vaccine breakthrough cases reported to CDC as of
June 21, 2021
More than 150 million people in US are fully vaccinated
During that time 4,115 patients with COVID-19 vaccine breakthrough infection were hospitalized (3,907) or died (750) .
Testimony In Front of Senate HHS Committee
1. A MATTER OF CONSCIENCE
Catholic-Vaccine and Conscience (Fr. Cristino Bouvette) February 10, 2021
CDC WHAT TO EXPECT AFTER YOUR COVID VACCINE
+++
FEMA CORONAVIRUS RUMOR CONTROL
Get Vaccinated
- Authorized COVID-19 vaccines can help protect you from COVID-19.
- You should get a COVID-19 vaccine when it is available to you.
- Once you are fully vaccinated, you may be able to start doing some things that you had stopped doing because of the pandemic.
- (However)
COVID-19 vaccines are effective at protecting you from getting sick. Based on what we know about COVID-19 vaccines, people who have been fully vaccinated can start to do some things that they had stopped doing because of the pandemic.
We’re still learning how vaccines will affect the spread of COVID-19. After you’ve been fully vaccinated against COVID-19, you should keep taking precautions in public places like wearing a mask, staying 6 feet apart from others, and avoiding crowds and poorly ventilated spaces until we know more.
Pregnant people are at increased risk for severe illness from COVID-19
Although the overall risk of severe illness is low, pregnant people are at an increased risk for severe illness from COVID-19 when compared to non-pregnant people. Severe illness includes illness that results in intensive care admission, mechanical ventilation, or death. Additionally, pregnant people with COVID-19 might be at increased risk of adverse pregnancy outcomes, such as preterm birth, compared with pregnant women without COVID-19.
(However see below)
Limited data are available about the safety of COVID-19 vaccines for people who are pregnant
Based on how these vaccines work in the body, experts believe they are unlikely to pose a specific risk for people who are pregnant. However, there are currently limited data on the safety of COVID-19 vaccines in pregnant people
- Clinical trials that look at the safety and how well the COVID-19 vaccines work in pregnant people are underway or planned.
- +++
Eugenio Derbez Interviews Dr. Fauci (March 13, 2021)
Anthony Fauci, M. D., NIAID Director (bio)
Dr. Fauci was appointed Director of NIAID in 1984. He oversees an extensive research portfolio of basic and applied research to prevent, diagnose, and treat established infectious diseases such as HIV/AIDS, respiratory infections, diarrheal diseases, tuberculosis and malaria as well as emerging diseases such as Ebola and Zika. NIAID also supports research on transplantation and immune-related illnesses, including autoimmune disorders, asthma and allergies. The NIAID budget for fiscal year 2021 is an estimated $6.1 billion. The video below with Professor Shane Crotty, PhD was recommended by Dr. Fauci.
US Grant to Wuhan Lab to Enhance Bat-Based Coronaviruses Was Never Scrutinized by HHS Review Board NIH Says - Daily Caller 4/4/21
4D. ARTICLES ON DR. FAUCI AND THE VACCINATION OF CHILDREN
White House Press Briefing Feb 19, 2021
If you look at the existing trials — those that have already gotten an EUA, and those that we anticipate and hope will get and EUA — when will we be able to say we can vaccinate children — children in the high school range and children in the elementary school range?
You know from Pfizer that they started off with the trial of 44,000 individuals, down to 16-year-olds and then progressed it down to 12-year-olds. So what they’re going to be doing in April — starting in April, they are going to be studying 12-year-olds down to five- to six-year-old. That will take likely one year to get the information on that — likely not until the first quarter.
However, we anticipate data on high-school-age individuals, namely individuals 12 years old to 17 years old, by the beginning of the fall. Maybe not exactly coinciding with the first day of school, but sometime in the fall, we will have that. Moderna, as you know, started off with already 18-year-old. They are now currently enrolling 12- to 17-year-olds.
Using Herd Immunity Excuse for Gene Therapy Vaccine on Kids March 18, 2021 - by Dr. Joseph Mercola
- Despite the fact that COVID-19 has had little impact, physically, to children, health officials are setting the stage for widespread vaccination of this population
- Considering that children are at extremely low risk from COVID-19, vaccination offers them far more risk than benefit, and parents understandably may be reluctant to volunteer their children to receive this experimental and unlicensed gene therapy
- Public health officials have made it clear, however, that vaccination of children is expected for the sake of herd immunity
- Studies suggest that children are not driving the COVID-19 pandemic and, in fact, appear less likely to transmit COVID-19 than adults
According to Children’s Health Defense (CHD), professor Dolores J. Cahill, Ph.D., a molecular biologist and immunologist, “expects to see successive waves of adverse reactions to the experimental messenger RNA (mRNA) injections ranging from anaphylaxis and other allergic responses to autoimmunity, sepsis and organ failure.”9
Considering that children are at extremely low risk from COVID-19, vaccination offers them far more risk than benefit, and parents may be understandably reluctant to volunteer their children to receive this experimental and unlicensed gene therapy. Public health officials have made it clear, however, that vaccination of children is expected. CHD reported:10
“Already last April — when next to nothing was known about COVID’s epidemiology, and candidate vaccines had barely begun to be studied — Bill Gates set the stage for the pediatric push, declaring that the end goal is to make COVID-19 vaccines 'part of the routine newborn immunization schedule.'”
Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases (NIAID), also stated that 85% to 90% of the U.S. population, including children, will need to receive a COVID-19 vaccine before life can return to normal, and he suggested that first graders may be authorized to be vaccinated by September 2021.
AAP News (March 17, 2021)
Dr. Fauci dismisses concerns about COVID-19 vaccines impacting children’s genetics
Children as young as first graders may be able to get the coronavirus vaccine by the time school starts in September, presuming trials are successful in those age groups, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, said in an interview with ProPublica.
“We’re in the process of starting clinical trials in what we call age de-escalation, where you do a clinical trial with people 16 to 12, then 12 to 9, then 9 to 6,” Fauci said. When asked what was the youngest age group that might be authorized for the vaccine by September, he said, “I would think by the time we get to school opening, we likely will be able to get people who come into the first grade.”
4E. MORE DR. FAUCI ON J & J
Which Does Dr Fauci Prefer: The Pfizer, Moderna, or Johnson & Johnson?
March 13, 2021 with Stephen Colbert
March 22, 2021 Dr. Fauci on the White House Website
Chief Medical Advisor to President Biden
on the Johnson and Johnson Vaccine
Dr. Fauci April 13, 2021 on the Johnson and Johnson Vaccine "Pause"
White House Press Conference
+++
Pfizer, a 171 year old Fortune 500 powerhouse, has made a billion-dollar bet on that dream.
For decades, scientists have dreamed about the seemingly endless possibilities of custom-made messenger RNA or mRNA. But turning scientific promise into medical reality has been more difficult than many assumed. Although relatively easy and quick to produce compared to traditional vaccine-making, no mRNA vaccine or drug has ever won approval.
And even though the studies by Karikó and Weissman went unnoticed by some, they caught the attention of two key scientists — one in the United States, another abroad — who would later help found Moderna and Pfizer’s future partner, BioNTech.
Within several months, Rossi, Langer, Afeyan, and another physician-researcher at Harvard formed the firm Moderna — a new word combining modified and RNA.
Springer was the first investor to pledge money, Rossi said. In a 2012 Moderna news release, Afeyan said the firm’s “promise rivals that of the earliest biotechnology companies over 30 years ago — adding an entirely new drug category to the pharmaceutical arsenal.”
But although Moderna has made each of the founders hundreds of millions of dollars — even before the company had produced a single product — Rossi’s account is marked by bitterness. In interviews with the Globe in October, he accused Langer and Afeyan of propagating a condescending myth that he didn’t understand his discovery’s full potential until they pointed it out to him.
Despite the squabbling that followed the birth of Moderna, other scientists also saw messenger RNA as potentially revolutionary.
In Mainz, Germany, situated on the left bank of the Rhine, another new company was being formed by a married team of researchers who would also see the vast potential for the technology, though vaccines for infectious diseases weren’t on top of their list then.
Both see themselves as scientists first and foremost. But they are also formidable entrepreneurs. After they co-founded another biotech, the couple persuaded twin brothers who had invested in that firm, Thomas and Andreas Strungmann, to spin out a new company that would develop cancer vaccines that relied on mRNA.
That became BioNTech, another blended name, derived from Biopharmaceutical New Technologies. Its U.S. headquarters is in Cambridge. Sahin is the CEO, Türeci the chief medical officer.
Moderna made a splash in 2012 with the announcement that it had raised $40 million from venture capitalists despite being years away from testing its science in humans. Four months later, the British pharmaceutical giant AstraZeneca agreed to pay Moderna a staggering $240 million for the rights to dozens of mRNA drugs that did not yet exist.
The biotech had no scientific publications to its name and hadn’t shared a shred of data publicly. Yet it somehow convinced investors and multinational drug makers that its scientific findings and expertise were destined to change the world. Under Bancel’s leadership, Moderna would raise more than $1 billion in investments and partnership funds over the next five years.
Moderna’s promise — and the more than $2 billion it raised before going public in 2018 — hinged on creating a fleet of mRNA medicines that could be safely dosed over and over. But behind the scenes the company’s scientists were running into a familiar problem. In animal studies, the ideal dose of their leading mRNA therapy was triggering dangerous immune reactions — the kind for which Karikó had improvised a major workaround under some conditions — but a lower dose had proved too weak to show any benefits.
Moderna had to pivot. If repeated doses of mRNA were too toxic to test in human beings, the company would have to rely on something that takes only one or two injections to show an effect. Gradually, biotech’s self-proclaimed disruptor became a vaccines company, putting its experimental drugs on the back burner and talking up the potential of a field long considered a loss-leader by the drug industry.
When BioNTech went public last October, it raised $150 million, and closed with a market value of $3.4 billion — less than half of Moderna’s when it went public in 2018.
Despite his role as CEO, Sahin has largely maintained the air of an academic. He still uses his university email address and rides a 20-year-old mountain bicycle from his home to the office because he doesn’t have a driver’s license.
Then, late last year, the world changed.
After isolating the virus from patients, Chinese scientists on Jan. 10 posted online its genetic sequence. Because companies that work with messenger RNA don’t need the virus itself to create a vaccine, just a computer that tells scientists what chemicals to put together and in what order, researchers at Moderna, BioNTech, and other companies got to work.
A pandemic loomed. The companies’ focus on vaccines could not have been more fortuitous.
Moderna and BioNTech each designed a tiny snip of genetic code that could be deployed into cells to stimulate a coronavirus immune response. The two vaccines differ in their chemical structures, how the substances are made, and how they deliver mRNA into cells. Both vaccines require two shots a few weeks apart.
Moderna was the first drug maker to deliver a potential vaccine for clinical trials. Soon, its vaccine became the first to undergo testing on humans, in a small early-stage trial. And on July 28, it became the first to start getting tested in a late-stage trial in a scene that reflected the firm’s receptiveness to press coverage.
The first volunteer to get a shot in Moderna’s late-stage trial was a television anchor at the CNN affiliate in Savannah, Ga., a move that raised eyebrows at rival vaccine makers.
Along with those achievements, Moderna has repeatedly stirred controversy.
On May 18, Moderna issued a press release trumpeting “positive interim clinical data.” The firm said its vaccine had generated neutralizing antibodies in the first eight volunteers in the early-phase study, a tiny sample.
But Moderna didn’t provide any backup data, making it hard to assess how encouraging the results were. Nonetheless, Moderna’s share price rose 20% that day.
Some top Moderna executives also drew criticism for selling shares worth millions, including Bancel and the firm’s chief medical officer, Tal Zaks.
In addition, some critics have said the government has given Moderna a sweetheart deal by bankrolling the costs for developing the vaccine and pledging to buy at least 100 million doses, all for $2.48 billion.
That works out to roughly $25 a dose, which Moderna acknowledges includes a profit.
Pfizer, through its partnership with BioNTech, isn’t taking any money upfront from the government. Rather, the federal government will pay the partners $1.95 billion for at least 100 million doses if the vaccine gets approved.
Some experts worry about injecting the first vaccine of this kind into hundreds of million of people so quickly.
“You have all these odd clinical and pathological changes caused by this novel bat coronavirus, and you’re about to meet it with all of these vaccines with which you have no experience,” said Paul Offit, an infectious disease expert at Children’s Hospital of Philadelphia and an authority on vaccines.
+++
6. PFIZER & MODERNA
PFIZER - The Facts about Pfizer and Biontech's COVID-19 Vaccine January 6, 2021 - Also see Pfizer main page here.
The Pfizer-BioNTech COVID-19 vaccine has not been approved or licensed by the U.S. Food and Drug Administration, but has been authorized for emergency use by FDA under an Emergency Use Authorization to prevent Coronavirus Disease 2019 for use in individuals 16 years of age and older. The emergency use of this product is only authorized for the duration of the declaration that circumstances exists justifying the authorization of emergency use of the medical product Section 564(b)(1) of the FD&C Act unless the declaration is terminated or authorization revoked sooner.
https://www.cvdvaccine.com/
The approval status of the Pfizer‑BioNTech COVID‑19 Vaccine varies worldwide. In countries where the vaccine has not been approved by the relevant regulatory authority, it is an investigational drug, and its safety and efficacy have not been established.
***Pfizer and BioNTech state High Efficacy and No Serious Safety Concerns through up to 6 months following second dose.***
+++
MODERNA - About the Moderna COVID-19 Vaccine
The Moderna COVID-19 Vaccine is an unapproved vaccine that has been authorized for emergency use by the FDA for active for emergency use by the FDA for active immunization to prevent COVID-19 in individuals 18 years of age and older. The vaccine was developed by Moderna, a biotechnology company that has focused on mRNA technology since 2010, and is currently being studied in a large Phase 3 trial.
+++
7. WORLD HEALTH ORGANIZATION - FATALITY RATE FROM COVID
Publication: Bulletin of the World Health Organization; Type: Research Article ID: BLT.20.265892 Page 1 of 37 John P A Ioannidis Infection Fatality Rate of COVID-19 (14 October 2020)
Abstract Objective To estimate the infection fatality rate of coronavirus disease 2019 (COVID-19) from seroprevalence data.
Results I included 61 studies (74 estimates) and eight preliminary national estimates. Seroprevalence estimates ranged from 0.02% to 53.40%. Infection fatality rates ranged from 0.00% to 1.63%, corrected values from 0.00% to 1.54%. Across 51 locations, the median COVID-19 infection fatality rate was 0.27% (corrected 0.23%): the rate was 0.09% in locations with COVID-19 population mortality rates less than the global average (< 118 deaths/million), 0.20% in locations with 118–500 COVID-19 deaths/million people and 0.57% in locations with > 500 COVID-19 deaths/million people. In people < 70 years, infection fatality rates ranged from 0.00% to 0.31% with crude and corrected medians of 0.05%.
Conclusion The infection fatality rate of COVID-19 can vary substantially across different locations and this may reflect differences in population age structure and case mix of infected and deceased patients and other factors. The inferred infection fatality rates tended to be much lower than estimates made earlier in the pandemic.
+++++++++++++++++++++++++++++
AND NOW A LOOK WHAT SOME OTHER DOCTORS SAY
+++++++++++++++++++++++++++++
8. DR. SIMONE GOLD - AMERICA FRONTLINE DOCTORS (linkedin)
Dr Simone Gold - The truth about the CV19 vaccine from Madeline Correia on Vimeo. February 2021
Apparently this video was censored. See the two Videos below with Dr. Gold. (8.8.2021)
And this video with Glen Beck
https://rumble.com/vgluk5-glenn-beck-doctor-exposes-the-real-reason....html
Link for the Lancet Retraction
+++
8a. America Frontline Doctors White Paper on COVID 19
+++
9. AMERICA FRONTLINE DOCTORS
How to Get COVID Medication
Ten Medical Facts Regarding the COVID-19
Experimental Vaccines by Shelley Cole (America Frontline Doctors)
America Frontline Doctors Homepage
The Biggest Experiment Ever Done
+++
11. ERRANT ANTIBODIES
Coronavirus vaccine developers wary of errant antibodies
Unfortunately the entire article is a paid version here is the summary of the News section of Nature Medicine, June 5, 2020, and written by Ken Garber:
This article explores a phenomenon called Antibody-Dependent Enhancement (ADE). This occurs when binding of a virus to non-neutralizing antibodies enhances its entry into host cells, and sometimes also its replication.
The clinical outcome in individuals where an immune response results in the production of non-neutralizing antibodies, either through natural infection or through vaccination, usually results in a more serious outcome after infection compared to those who are immunologically naive.
Prior observations of ADE in some early SARS and MERS vaccine candidates recommends consideration of vaccine design and extensive animal testing as we move forward with clinical trials for vaccines directed against SARS-CoV-2.
"…There are mounting theoretical concerns that vaccines generating antibodies against SARS-CoV-2 may bind to the virus without neutralizing it. Should this happen, the non-neutralizing antibodies could enhance viral entry into cells and viral replication and end up worsening infection instead of offering protection, through the poorly understood phenomenon of ADE. ADE “is a genuine concern,” says virologist Kevin Gilligan, a senior consultant with Biologics Consulting, who advises thorough safety studies. “Because if the gun is jumped, and a vaccine is widely distributed that is disease enhancing, that would be worse than actually not doing any vaccination at all.”
+++
12. LONG-TERM VACCINE EFFECTS INFLAMMATION-INDUCED DISRUPTIONS
+++
13. WORLD HEALTH ORGANIZATION - INFECTION RATE AFTER VACCINE
World Health Organization - COVID19 Virtual Press Conference - December 28, 2020
TJ Thank you very much, Professor Koopmans. Let’s try to take a couple more questions, although we are already nearing the hour marker. Let’s go to Sydney Morning Herald, and we have Latika Bourke with us. Latika?
LB Thank you so much. Thank you for being with us today, and for taking these questions. I’m particularly interested in your views on how you think the vaccine will work in the context of elimination, because countries in my home patch, of course, in the Asia-Pacific, have done very well and kept community transmission rates very low, to the point where some have eliminated.
But what does that mean for in the long-term, where people are vaccinated overseas? Does that ensure that they are not a risk, traveling to countries that have almost zero community transmission? Or do you think that people who have been vaccinated will still need to quarantine if they’re going to countries that have low transmission?
TJ That’s an excellent question, Latika. Thank you very much for that. I’ll ask Dr Swaminathan if she can answer this question. Dr Swaminathan.
SS Thank you. And others might want to add, but I think that’s a really important question. And I think, Latika, what we’re learning now, and we continue to wait for more results from the vaccine trials, is to really understand if these vaccines, apart from preventing symptomatic disease and severe disease and deaths, whether they’re also going to reduce infections, or prevent people from getting infected with the virus, prevent them from passing it on or transmitting it to other people.
01:00:03
At the moment, I don’t believe we have the evidence on any of the vaccines to be confident that it’s going to prevent people from actually getting the infection and therefore being able to pass it on. So, I think until we know more, we need to assume that people who have been vaccinated also need to take the same precautions until there is a certain level of herd immunity, of course, that’s been built in the population. So, again, this is a dynamic and evolving field, and I think our understanding and our recommendations will change as we get more follow-up data from these trials. Thanks. Others might want to add.
TJ Thank you very much, Dr Swaminathan. Dr Ryan?
MR No, I agree with Soumya’s points there. And I think it’s important that we also reflect on that the main objective of the vaccine and the first rollout will be to prevent severe illness, to prevent deaths, to protect frontline health workers, and to protect the most vulnerable people in our society.
And we would hope that that protection is offered to health workers and vulnerable people all around the world. So the first and primary objective is to decrease the impact that this disease is having on people’s lives. And therefore, that will be a major step forward in bringing the world back to some kind of normal.
01:01:30
The second phase is then looking at how will this vaccine affect transmission. And Soumya is right. We just don’t know enough yet about length of protection and other things to be absolutely able to predict that. But I think we should be able to get good control of the virus.
A decision then to move towards elimination or eradication of the virus requires a much higher degree of efficiency and effectiveness in a vaccination programme and all of the other control measures. And we still don’t know, based on virus evolution, based on so many other things.
The likely scenario is the virus will become, as David Heymann said previously, another endemic virus, a virus that will remain somewhat of a threat, but a very low-level threat in the context of an effective global vaccination programme. We will have to… It remains to be seen how well the vaccines are taken up, how close we get to a coverage level that might allow us the opportunity to go for elimination or eradication.
We’ve seen this with polio. We’ve seen this with measles. So, Bruce and others online, Ana Maria and others who have a lot of experience with measles and polio may be able to speak about this. The existence of a vaccine, even at high efficacy, is no guarantee of eliminating or eradicating an infectious disease. That is a very high bar for us to be able to get over.
First and foremost, we have to focus on saving lives, getting good control on this epidemic so our societies can return to normal, and then we will deal with the moon-shot of potentially being able to eliminate or eradicate this virus. But at this point, based on the tools we have and the knowledge we have, that’s impossible to say at this moment.
+++
14. WILL VACCINES SAVE LIVES?
Will COVID-19 Vaccines Save Lives? Current Trials Aren't Designed to Tell Us
October 21, 2020 (The BMJ)Article at a glance:As phase III trials of covid-19 vaccines reach their target enrolments, officials have been trying to project calm. The US coronavirus czar Anthony Fauci and the Food and Drug Administration leadership have offered public assurances that established procedures will be followed. Only a “safe and effective” vaccine will be approved, they say, and nine vaccine manufacturers issued a rare joint statement pledging not to prematurely seek regulatory review.
But what will it mean exactly when a vaccine is declared “effective”? To the public this seems fairly obvious. “The primary goal of a covid-19 vaccine is to keep people from getting very sick and dying,” a National Public Radio broadcast said bluntly.
Peter Hotez, dean of the National School of Tropical Medicine at Baylor College of Medicine in Houston, said, “Ideally, you want an antiviral vaccine to do two things . . . first, reduce the likelihood you will get severely ill and go to the hospital, and two, prevent infection and therefore interrupt disease transmission.”
Yet the current phase III trials are not actually set up to prove either. None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.
+++
15. COVID-19 VACCINE SIDE EFFECTS
CONCERNED DOCTORS SPEAK OUT
See Full Article Here This is an excerpt from an analysis done March 23, 2021
If early statistics are any indication, we are facing the greatest public health calamity in modern history. No, I’m not talking about a third, fourth or fifth wave of COVID-19. I’m talking about the current vaccination campaign. I have no doubt that deaths caused by COVID-19 vaccines will end up far exceeding the number of actual COVID-19 deaths.
The greatest tragedy here is that while COVID-19 kills already unhealthy elderly individuals who are just years from their natural death, the vaccines are killing the young and healthy who typically have many more decades to live. From my perspective, there’s simply no justification for this. There’s no “greater good” argument that can ever make this type of tradeoff OK.
Equally unjustifiable is the fact that death within months of a positive SARS-CoV-2 test was automatically pegged as a COVID-19 death, whereas death within days or even hours of the vaccine is shrugged off as coincidental, no matter how many times it happens. It is reprehensibly inexcusable the way these deaths are being attributed.
Now, these experimental gene therapy “vaccines” are being tested on young children and even babies as young as 6 months old, the ramifications of which are wholly unknown.
According to Forbes1 and The New York Times,2 Moderna has officially started testing its vaccine on children between the ages of 6 months and 11 years. A total of 6,750 children will be included in the trial. Testing on 12- to 17-year-olds began in December 2020, the data from which are still unpublished. Considering what’s happening in the adult population, testing on young children and babies seems extremely premature and risky beyond belief.
Comparing COVID-19 and Vaccine Death Rates
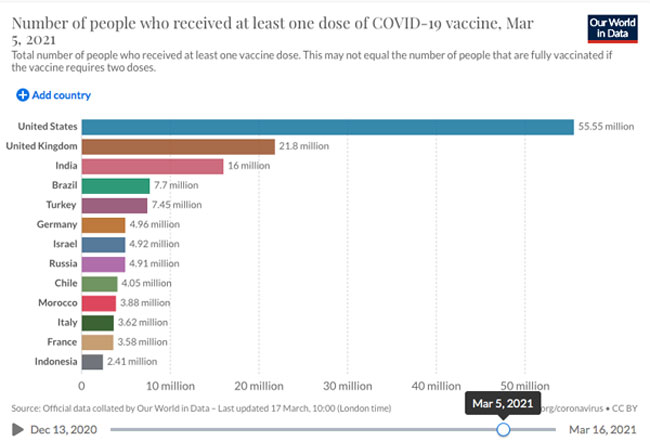
Another difficulty is matching different data sets together. For example, to put these numbers into greater context, you’d want to know how many people have been vaccinated as of that same date, March 5, 2021.
This too can be tricky to determine, as vaccination statistics will often use breakdowns such as the number of vaccinated people per 100, or vaccine doses administered, which doesn’t tell you how many people were vaccinated, seeing how some vaccines require a single dose while others require two.
Accepting those limitations, we can at least get an approximate idea. Using Our World in Data’s statistics,7 as of March 5, 2021, 55.55 million Americans had received at least one dose. (Another graph shows that as of March 5, 28.7 million Americans were considered fully vaccinated, having received all prescribed doses. However, since side effects can occur after the first dose, I will use that statistic.)
Dividing reported deaths, 1,551, by the number of people having received at least one dose, 55,550,000, we end up with a reported lethality rate of 0.0028%. If only 10% of adverse events are reported to VAERS, we’re looking at approximately 15,510 deaths and a lethality rate of 0.028%.
If only 1% are reported, there may be around 155,100 deaths, and vaccines may be killing 0.28% of all who get them. Again, while any and all deaths following COVID-19 vaccination are supposed to be reported, it’s still unclear whether mandatory reporting is actually taking place.
While 0.0028% or even 0.28% might not seem like a shockingly high percentage of deaths, it’s hard to justify even a single death of a young and healthy individual. For comparison, the overall noninstitutionalized infection fatality ratio from COVID-19, for all age groups, is 0.26%. Those under 40 have only a 0.01% risk of dying from COVID-19 if infected.8
As of right now, the vaccine may not match or exceed the lethality of COVID-19 itself, but we’re only three months into the vaccination campaign. According to NPR,9 21.7% of the U.S. population had received at least one vaccine dose as of March 16, 2021.
There are compelling reasons to suspect these vaccines may contribute to death further down the line, perhaps months or a few years into the future. Those ending up with permanent disability as a result of these vaccines will be at increased risk of early death, for example, and there’s no telling how these vaccines might impact the longevity of children.
If premature death occurs a year or more down the line, it’s unlikely that anyone will suspect it being connected to the vaccine. Right now, even deaths that occur within 24 hours in people who were young and in good health are chalked up to coincidence, which is truly remarkable.
Comparing COVID-19 Vaccines With Flu Vaccines
Another way to judge the lethality of COVID-19 vaccines is to compare it to seasonal flu vaccines which, by the way, used to account for a majority of vaccine injuries. As reported by The Vaccine Reaction:10
“The death rate following COVID mRNA vaccination is much higher than that following influenza vaccination. The CDC’s data allows only a ballpark estimation of the rate of deaths following flu vaccination. In the 2019-2020 influenza season the CDC reports that 51.8 percent of the U.S. population received a vaccine, which is approximately 170 million people.
VAERS reports that in the calendar year 2019 (not the 2019-2020 influenza season) there were 45 deaths following vaccination. To provide context, in 2018 VAERS reports 46 deaths, and in 2017 it reports 20 deaths.
The 45 deaths in 2019 are occurring at a rate of 0.0000265% when calculated using the number of vaccines given in the 2019–2020 influenza season. As of Feb. 26, 47,184,199 COVID vaccinations had been given with 1,136 deaths reported following vaccination, which is approximately a rate of .0024%.”
Are These Deaths Pure Coincidence?
As of March 5, 2021, the youngest recorded death shortly following COVID-19 vaccination was 23.11 Among the more recent reports is that of a healthy 39-year-old mother who died of multiple organ failure just four days after receiving her second dose of the Moderna vaccine.12
The average age of death post-vaccination is 75 and older,13 which is near-identical to the age of death for COVID-19 itself. However, whereas COVID-19 primarily kills elderly in nursing homes who have multiple comorbidities, the vaccines are cutting lives short among elderly who appear to be in relatively good health.
Examples include baseball legend Hank Aaron, who died in his sleep 17 days after receiving the vaccine. He was 86. His death was reported as completely natural and unrelated to the vaccine.14
Another is that of boxing champ Marvin Hagler who, according to his friend Thomas Hearns, was admitted to the ICU due to side effects from his COVID-19 vaccination. (Hearns had posted on his Instagram and Twitter accounts that Hagler was in the hospital ICU “fighting the after effects of the vaccine” and that he wanted fans to pray for his recovery.15
His posts have since been removed, but a screenshot of a retweet16 by Tariq Nasheed is still available.) Hagler died shortly thereafter. He was 66.
I suspect that once more celebrities start dying from the vaccines, more people might start to rethink their decision to get vaccinated. Mainstream media and industry-allied fact checkers are working overtime, though, to “debunk” any suggestion of a link between deaths and the vaccines.
Side Effects Range From Mild to Serious
Aside from sudden death,17,18,19,20,21,22 which is most serious of all, a range of other side effects are being reported, many of which will have a significant impact on quality of life. Examples of side effects reported after vaccination with Pfizer’s, Moderna’s and AstraZeneca’s vaccines from around the world include:
Persistent malaise23,24 | Bell’s Palsy25,26,27 |
Extreme exhaustion28 | Swollen, painful lymph nodes |
Severe allergic, including anaphylactic reactions29,30,31 | Thrombocytopenia (a rare, often lethal blood disorder)32,33 |
Multisystem inflammatory syndrome34 and/or myocarditis35 | Miscarriages and premature birth.36,37,38 As of March 5, 2021, 85 cases of miscarriage or premature birth had been reported39 |
Chronic seizures and convulsions40,41 | Severe headache/migraine that does not respond to medication |
Paralysis42 | Sleep disturbances |
Psychological effects such as mood changes, anxiety, depression, brain fog, confusion, dissociation and temporary inability to form words | Cardiac problems, including myocardial and tachycardia disorders43 |
Blindness, impaired vision and eye disorders44,45 | Stroke46,47 |
As reported by The Defender, March 5, 2021, while vaccine injury reports are growing in number, consistent trends have emerged, including the following:48
- Overall, 31% of deaths have occurred within 48 hours of vaccination
- People who report getting sick within 48 hours of vaccination account for 47% of deaths
- About 20% of deaths are cardiac-related
A majority of these side effects are from the Moderna and Pfizer vaccines, which use mRNA technology. The AstraZeneca vaccine uses a chimpanzee adenovirus vector genetically engineered to express the SARS-CoV-2 spike protein instead. However, while many hoped this vaccine would be safer than mRNA versions, this doesn’t seem to be the case.
As of March 16, 2021, more than 20 European countries had suspended the use of AstraZeneca’s vaccine, either in full or in part, following reports of deadly blood clots.49,50 According to a March 2, 2021, report51 by The Defender, U.K. data show the AstraZeneca vaccine actually has 77% more adverse events and 25% more deaths than the Pfizer vaccine.
Like AstraZeneca’s vaccine, Johnson & Johnson’s vaccine also uses an adenovirus vector to carry the gene for SARS-CoV-2 spike protein into your cells, thereby triggering your cells to produce this protein.52 Business Insider has created a comparison chart53 of the four vaccines currently available in the U.S. and Europe — Moderna, Pfizer, AstraZeneca and Johnson & Johnson.
Concerned Doctors Speak Out
Sadly, the vaccine debate is nothing if not one-sided. Medical professionals expressing concern are roundly ignored, despite their growing number. Among them is cardiac surgeon and patient advocate Dr. Hooman Noorchashm, who recently sent a public letter54 to the U.S. Food and Drug Administration commissioner detailing the risks of vaccinating individuals who have previously been infected with SARS-CoV-2, or who have an active SARS-CoV-2 infection.
He’s urging the FDA to require prescreening for SARS-CoV-2 viral proteins to reduce the risk of injuries and deaths following vaccination. He warns the vaccine may trigger an adverse immune response in those who have already been infected with the virus.
Immunologist Dr. Bart Classen has also warned there is troubling evidence suggesting some mRNA shots may cause prion diseases such as Alzheimer’s and ALS,55 and Dr. J. Patrick Whelan, a pediatric rheumatologist specializing in multisystem inflammatory syndrome, has expressed concern about mRNA vaccines’ ability to cause “microvascular injury to the brain, heart, liver and kidneys in ways that were not assessed in safety trials.”56
16. ARE COVID19 VACCINES GENE THERAPY?
COVIC-19 'Vaccines' Are Gene Therapy - Analysis by Dr. Joseph Mercola (March 16, 2021)
Story at a glance:
- mRNA “vaccines” created by Moderna and Pfizer are gene therapies. They fulfill all the definitions of gene therapy and none of the definitions for a vaccine. This matters, as you cannot mandate a gene therapy against COVID-19 any more than you can force entire populations to undergo gene therapy for a cancer they do not have and may never be at risk for
- mRNA contain genetic instructions for making various proteins. mRNA “vaccines” deliver a synthetic version of mRNA into your cells that carry the instruction to produce the SARS-CoV-2 spike protein, the antigen, that then activates your immune system to produce antibodies
- The only one benefiting from an mRNA “vaccine” is the vaccinated individual, since all they are designed to do is lessen clinical symptoms associated with the S-1 spike protein. Since you’re the only one who will reap a benefit, it makes no sense to demand you accept the risks of the therapy “for the greater good” of your community
- Since mRNA “vaccines” do not meet the medical and/or legal definition of a vaccine, marketing them as such is a deceptive practice that violates the law that governs advertising of medical practices
- SARS-CoV-2 has not even been proven to be the cause of COVID-19. So, a gene therapy that instructs your body to produce a SARS-CoV-2 antigen — the viral spike protein — cannot be said to be preventive against COVID-19, as the two have not been shown to be causally linked (Link to entire article above)
+++
17. WHAT IS HERD IMMUNITY?
I googled WebMD for my answer:
With the rising number of cases of COVID-19 around the world, health officials continue to work to find the best way to protect the public from the disease. You may have heard health officials mention herd immunity as a possible way to contain the spread of COVID-19.
Here’s what you need to know about herd immunity and how it may help slow the spread of the new coronavirus.
Herd Immunity
Herd immunity, or community immunity, is when a large part of the population of an area is immune to a specific disease. If enough people are resistant to the cause of a disease, such as a virus or bacteria, it has nowhere to go.
While not every single individual may be immune, the group as a whole has protection. This is because there are fewer high-risk people overall. The infection rates drop, and the disease peters out.
Herd immunity protects at-risk populations. These include babies and those whose immune systems are weak and can’t get resistance on their own.
How Do You Achieve Herd Immunity?
There are two ways this can happen.
You can develop resistance naturally. When your body is exposed to a virus or bacteria, it makes antibodies to fight off the infection. When you recover, your body keeps these antibodies. Your body will defend against another infection. This is what stopped the Zika virus outbreak in Brazil. Two years after the outbreak began, 63% of the population had had exposure to the virus. Researchers think the community reached the right level for herd immunity.
Vaccines can also build resistance. They make your body think a virus or bacteria has infected it. You don’t get sick, but your immune system still makes protective antibodies. The next time your body meets that bacteria or virus, it’s ready to fight it off. This is what stopped polio in the United States.
When does a community reach herd immunity? It depends on the reproduction number, or R0. The R0 tells you the average number of people that a single person with the virus can infect if those people aren’t already immune. The higher the R0, the more people need to be resistant to reach herd immunity.
Researchers think that the R0 for COVID-19 is between 2 and 3. This means that one person can infect two to three other people. It also means 50% to 67% of the population would need to be resistant before herd immunity kicks in and the infection rates start to go down.
+++
18. WE ARE GOING TO PAY A HUGE PRICE FOR MASS COVID VACCINATIONS - REBUTTAL BELOW
Virologist: 'We Are Going to Pay Huge Price' for COVID Mass Vaccination Campaign by Children's Health Defense Team (3/15/21)
Bossche says that a mass vaccination campaign in the middle of a pandemic, with vaccines that don’t prevent transmission, is disastrous at an individual — and at a global — level:
“We are going to pay a huge price for this. And I’m becoming emotional because I’m thinking of my children, of the younger generation. I mean, it’s just impossible what we are doing. We don’t understand the pandemic.”
In an open letter to the World Health Organization (WHO), Bossche wrote that “we are currently turning vaccinees into asymptomatic carriers shedding infectious variants.”
Bossche hasn’t heard back from WHO, which concerns him.
“It is about humanity … I mean, it’s about your children. It’s your family. It’s my family. It’s everyone. Right. And it’s simply for me, I put everything at stake because I’ve done my homework. And this is simply a moral obligation. A moral obligation.”
Mass Vaccination in a Pandemic - Benefits v. Risks: Geert Vanden Bossche (bio)
Rebuttal: The 'Not-So-Hidden Agenda' Behind Bossche's Concern Over COVID Mass Vaccination - Rosemary Frei, MSc.
+++
20. DR. SUNEEL DHAND - MedStoic LIFESTYLE MEDICINE
Why I Haven't Taken the COVID Vaccine Yet
+++
Nurse's father dies after having COVID and then taking the shot
29. CDC Finds 'LIkely' Link between Heart Inflammation and Pfizer, Moderna COVID Vaccines (The Defender 6.23.21)
In this interview, return guest Dr. Vladimir Zelenko discusses an incredibly serious concern, one shared with at least two other highly credible experts — Michael Yeadon, Ph.D., a life science researcher and former vice-president and chief scientist of allergy and respiratory research at Pfizer, and professor Luc Montagnier, a world-renowned virologist who won the Nobel prize for his discovery of HIV.
Yeadon, Montagnier and Zelenko all believe the COVID-19 shots could reduce life expectancy by several decades, depending on several factors, including whether you’re required to get booster shots. In fact, there may be reason to suspect that many who get the jabs and subsequent boosters could lose their lives within two to three years, as a result of pathogenic priming.
Interview with virologist Dr. Sucharit Bhakdi (bio) on why the rushed COVID-19 vaccine trials represent one of the world's largest medical experiments. Dr. Bhakdi is an award-winning virologist with 300 published articles on immunology, bacteriology, virology and parasitology. (Video on link)